Medication Administration Record Sheet PDF Form
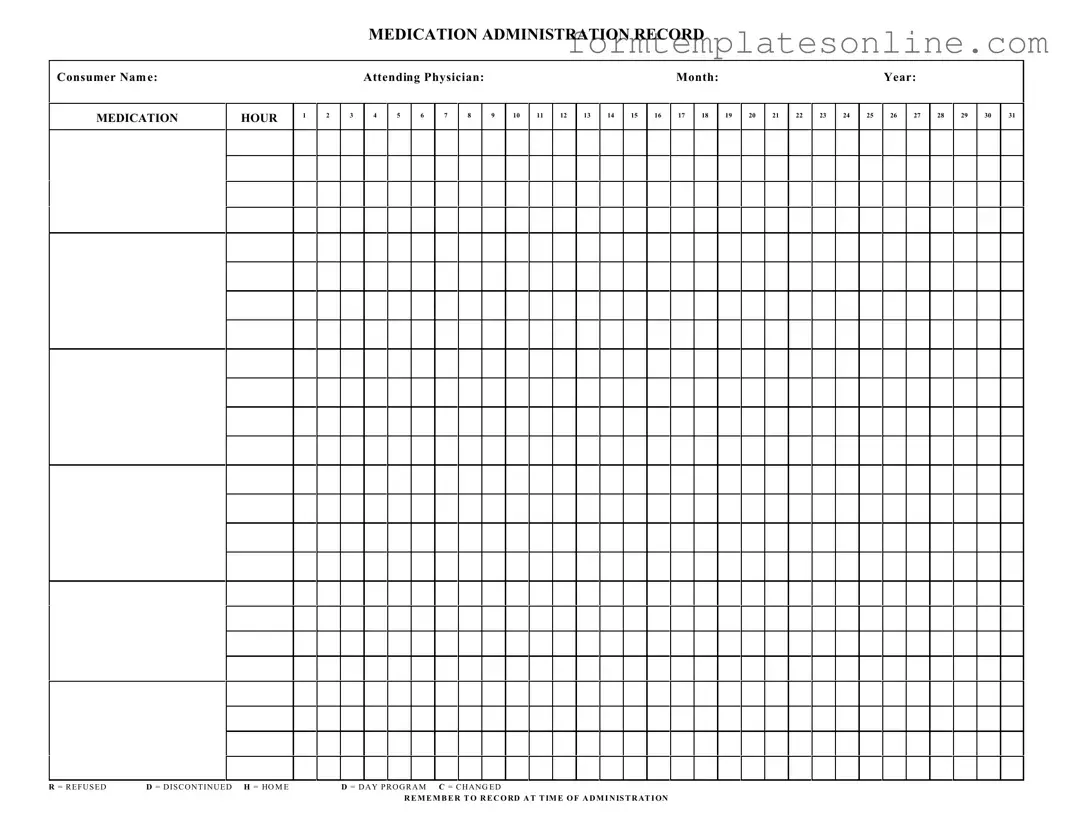
The Medication Administration Record Sheet (MARS) is a crucial tool in the healthcare setting, designed to ensure the accurate and timely administration of medications to patients. This form captures essential details, including the consumer's name, attending physician, and the specific month and year of administration, providing a comprehensive overview of a patient's medication regimen. Each hour of the day is meticulously outlined, allowing healthcare providers to record the administration of medications at precise intervals. The MARS also includes specific notations such as "R" for refused medications, "D" for discontinued treatments, "H" for home medications, and "C" for any changes made to the prescribed regimen. This structured approach not only facilitates effective communication among healthcare professionals but also enhances patient safety by ensuring that all medication-related actions are documented accurately. Furthermore, it serves as a reminder to healthcare providers to record each administration at the designated time, thereby promoting accountability and adherence to prescribed treatment plans.
Common mistakes
-
Not including the consumer name at the top of the form. This can lead to confusion about which patient the record pertains to.
-
Failing to specify the attending physician. Without this information, it may be unclear who is responsible for the medication plan.
-
Leaving the month and year blank. This omission can create issues when tracking medication history over time.
-
Incorrectly marking the medication hours. Accurate timing is crucial for proper medication administration and monitoring.
-
Not recording the status of the medication, such as refused, discontinued, or changed. This information is vital for understanding a patient’s medication adherence.
-
Forgetting to record at the time of administration. Timely documentation helps ensure accuracy and accountability in medication management.
Example - Medication Administration Record Sheet Form
MEDICATION ADMINISTRATION RECORD
Consumer Nam e:
MEDICATION
HOUR
1
2
|
Attending Physician: |
|
|
|
|
|
|
|
|
Month: |
|
|
|
|
|
|
|
Year: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
5 |
6 |
7 |
8 |
|
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
|
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
29 |
30 |
31 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R = R E F U S E D |
D = D I S C O N T I N U E D H = HO M E |
D = D A Y P R O G R A M C = C H A N G E D |
R E M E M B E R T O R E C O RD A T T IM E O F A D M I N IS T R AT I ON
More About Medication Administration Record Sheet
What is a Medication Administration Record Sheet?
The Medication Administration Record Sheet is a document used to track the administration of medications to consumers. It ensures that all doses are recorded accurately, helping to maintain a clear history of medication use for each individual. This sheet is essential for healthcare providers to monitor patient compliance and medication effectiveness.
How do I fill out the Medication Administration Record Sheet?
To fill out the sheet, begin by entering the consumer's name, the attending physician's name, and the date (month and year). Then, for each medication administered, mark the appropriate hour and date. Use the designated codes to indicate if a dose was refused (R), discontinued (D), or if there was a change (C). Always record the information at the time of administration to ensure accuracy.
What do the codes on the form mean?
The codes are shorthand notations used to indicate specific actions regarding medication administration. 'R' stands for Refused, meaning the consumer did not take the medication. 'D' indicates Discontinued, which means the medication is no longer being administered. 'H' refers to Home, while 'D' can also denote Day Program. 'C' indicates that there has been a Change in the medication. These codes help maintain clarity and consistency in record-keeping.
Why is it important to record medication administration at the time it occurs?
Recording medication administration at the time it occurs is crucial for maintaining accurate medical records. This practice helps prevent errors, such as double dosing or missing doses, and provides a reliable account of the consumer's medication history. Timely documentation also aids healthcare providers in making informed decisions regarding ongoing treatment.
Who is responsible for filling out the Medication Administration Record Sheet?
The responsibility for filling out the Medication Administration Record Sheet typically falls on healthcare providers, such as nurses or caregivers, who administer the medications. It is important that those responsible for documentation are trained in proper record-keeping practices to ensure accuracy and compliance with regulations.
What should I do if a medication is refused?
If a consumer refuses a medication, you should mark the appropriate hour and date with an 'R' on the Medication Administration Record Sheet. Additionally, it is important to document the reason for refusal, if known, and notify the attending physician. This information can help in adjusting the treatment plan if necessary.
Can changes to medication be noted on this form?
Yes, changes to medication can be noted on the Medication Administration Record Sheet. When a medication is changed, you should mark the hour and date with a 'C' to indicate that a change has occurred. It is also advisable to document the details of the change in the consumer's medical record to provide comprehensive information for future reference.
How long should the Medication Administration Record Sheet be kept?
The Medication Administration Record Sheet should be kept for a minimum period as specified by state regulations or organizational policies. Generally, it is advisable to retain these records for several years to ensure compliance with legal and medical standards. Always check with your organization’s guidelines for specific retention policies.
What should I do if I make an error on the Medication Administration Record Sheet?
If an error is made on the Medication Administration Record Sheet, it is important to correct it properly. Cross out the incorrect entry with a single line, and write the correct information next to it. Initial the correction and date it to maintain a clear record of changes. Avoid using correction fluid or erasers, as this can obscure the original entry.
Key takeaways
When using the Medication Administration Record Sheet form, consider the following key takeaways:
- Accurate Information: Ensure that the consumer's name, attending physician, month, and year are correctly filled out at the top of the form.
- Timely Recording: Record the administration of medication at the time it is given. This helps maintain accurate records.
- Use of Codes: Familiarize yourself with the codes for recording medication status, such as R for refused and D for discontinued.
- Hourly Tracking: Pay attention to the hourly sections on the form. Each hour should be marked clearly to indicate when medication is administered.
- Changes and Notes: If there are any changes in medication or specific notes, document them in the appropriate sections to ensure clear communication.
Form Attributes
| Fact Name | Description |
|---|---|
| Consumer Name | The form requires the name of the consumer receiving medication. |
| Attending Physician | The name of the physician responsible for the consumer's care must be included. |
| Medication Hours | There are designated hours for medication administration, labeled 1 through 24. |
| Monthly Record | The form is structured to track medication for a specific month and year. |
| Refusal and Discontinuation Codes | Codes R (Refused) and D (Discontinued) are used to indicate medication status. |
| Home and Day Program Codes | Codes H (Home) and D (Day Program) clarify the setting of medication administration. |
| Change Code | The code C (Changed) is utilized when there is a modification in the medication regimen. |
| Documentation Requirement | It is essential to record the administration time for each medication given. |
| State-Specific Regulations | Each state may have specific laws governing the use of the Medication Administration Record. |
| Legal Compliance | Failure to accurately complete the form may result in legal and regulatory consequences. |
Other PDF Forms
Employee Advance Repayment Agreement - The form helps clarify the situation surrounding the advance request for both parties.
Create Own Invoice - A customizable template for creating invoices effortlessly.
Having the proper documentation is essential for any transaction, and when it comes to buying or selling a trailer in Georgia, the Trailer Bill of Sale form is necessary. It ensures transparency by providing a record of the sale, including essential details such as the purchase price and trailer specifics. For further assistance in understanding or obtaining this important document, you may visit OnlineLawDocs.com.
Minor Child Travel Consent Form Notarized - The consent form addresses potential health and safety issues regarding minors on board.
Dos and Don'ts
When filling out the Medication Administration Record Sheet form, it is crucial to ensure accuracy and clarity. Here are some important dos and don'ts to consider:
- Do write clearly and legibly to avoid any misinterpretation.
- Do include the consumer's full name at the top of the form.
- Do record the date accurately to maintain a proper timeline of medication administration.
- Do note the attending physician's name for reference.
- Don't leave any blank spaces; fill in all required fields to ensure completeness.
- Don't use abbreviations that could be misunderstood; clarity is key.
- Don't forget to record the time of administration as specified in the instructions.