DD 2870 PDF Form
The DD 2870 form plays a crucial role in the military healthcare system, specifically in the realm of obtaining and sharing medical records. This form is primarily used by service members, veterans, and eligible dependents to authorize the release of their health information. Understanding the importance of this document is essential for anyone navigating the complexities of military healthcare. It ensures that medical providers can access necessary records, which is vital for delivering appropriate care. Additionally, the DD 2870 serves as a protective measure, safeguarding personal health information while allowing for the seamless transfer of data between authorized entities. Whether you're a service member seeking treatment or a healthcare provider needing access to patient records, familiarity with the DD 2870 form can streamline processes and enhance the quality of care received. As you delve into this article, you'll discover not only how to complete the form but also the implications of its use in various healthcare scenarios.
Common mistakes
-
Not providing accurate personal information. Ensure that names, addresses, and contact details are correct.
-
Failing to sign the form. A signature is required to validate the submission.
-
Leaving out the date. Always include the date when the form is completed.
-
Neglecting to check for required documentation. Some sections may need additional documents attached.
-
Using incorrect or outdated versions of the form. Always download the latest version from the official source.
-
Providing incomplete information in the sections. Each section must be fully filled out to avoid delays.
-
Not following instructions carefully. Read the guidelines provided with the form to ensure compliance.
-
Submitting the form to the wrong address. Confirm the correct submission location based on your circumstances.
-
Overlooking the need for witnesses or notary. Some submissions may require additional verification.
-
Failing to keep a copy of the submitted form. Always retain a copy for your records.
Example - DD 2870 Form
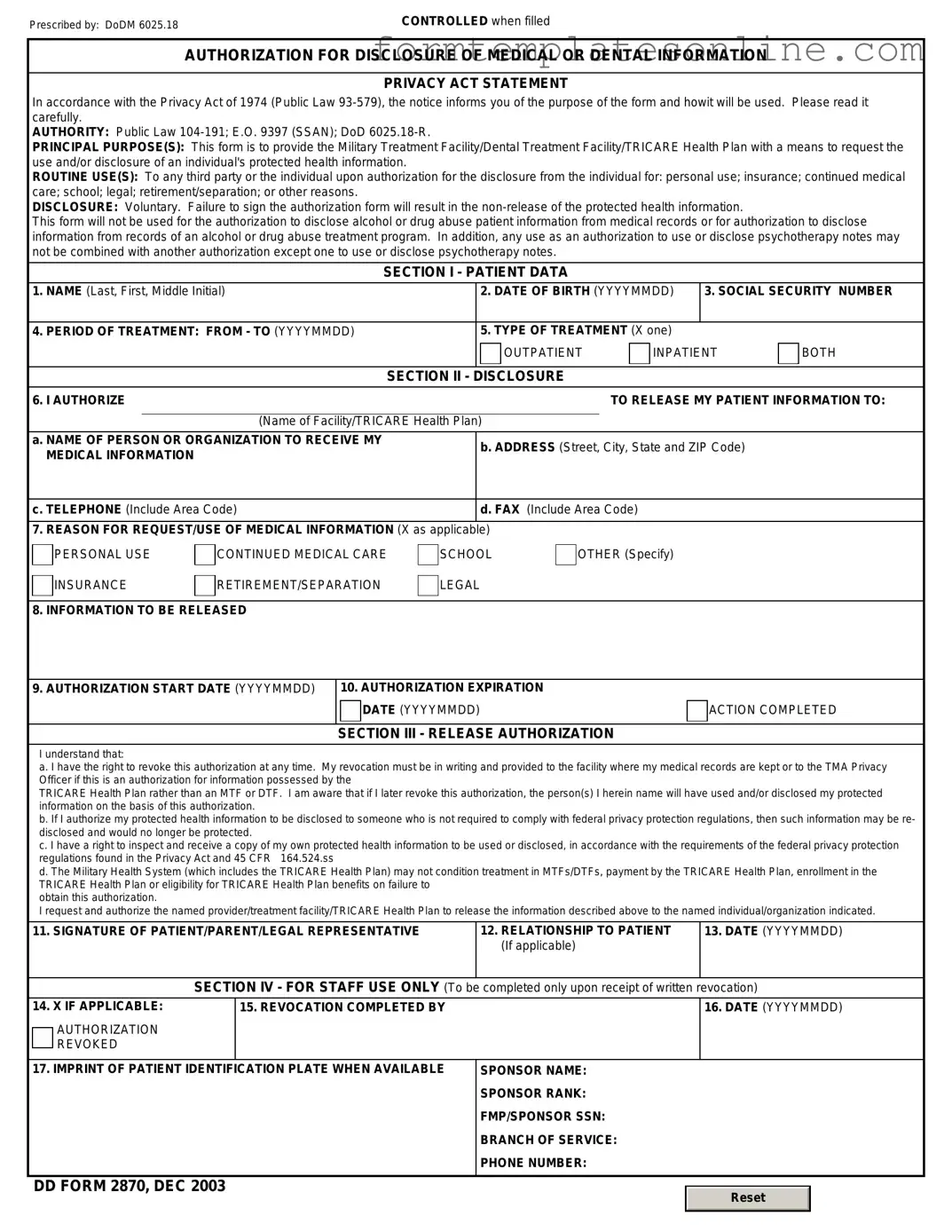
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
More About DD 2870
What is the DD 2870 form?
The DD 2870 form, also known as the "Authorization for Disclosure of Medical or Dental Information," is a document used by military personnel and their dependents. It allows individuals to authorize the release of their medical or dental records to specified parties. This form is essential for ensuring that medical information is shared appropriately while maintaining privacy standards.
Who needs to fill out the DD 2870 form?
Any active duty member of the military, reservists, retirees, and their dependents may need to complete the DD 2870 form when they wish to authorize the release of their medical or dental information. This could be necessary for various reasons, including seeking treatment from civilian healthcare providers or for insurance purposes.
Where can I obtain the DD 2870 form?
The DD 2870 form can be obtained from various sources. It is available online through the official Department of Defense website or the military branch's healthcare facility. Additionally, service members can request a copy from their unit's administrative office or medical records department.
How do I fill out the DD 2870 form?
Filling out the DD 2870 form involves providing personal information, including the individual's name, Social Security number, and contact information. The form also requires the name of the person or organization receiving the medical records, along with the specific information that is being authorized for release. Clear instructions are provided on the form to guide users through the process.
Is there a specific format for submitting the DD 2870 form?
The DD 2870 form can typically be submitted in person at the appropriate medical facility or sent via mail. Some facilities may also allow electronic submissions. It is advisable to check with the specific healthcare provider for their preferred submission method to ensure timely processing.
How long does it take to process the DD 2870 form?
The processing time for the DD 2870 form can vary depending on the healthcare facility and the volume of requests. Generally, it may take several days to a few weeks to process the authorization and release the requested medical or dental records. Individuals are encouraged to follow up with the facility if there are concerns about delays.
Can I revoke the authorization after submitting the DD 2870 form?
Yes, individuals have the right to revoke their authorization at any time. To do so, a written request should be submitted to the same office where the DD 2870 form was submitted. It is important to specify that the authorization is being revoked to ensure that no further information is released.
What happens if I do not complete the DD 2870 form?
If the DD 2870 form is not completed, medical or dental records cannot be released to the specified party. This may impact the ability to receive necessary care from outside providers or to process insurance claims that require medical documentation. Completing the form is crucial for the appropriate sharing of health information.
Are there any fees associated with the DD 2870 form?
Generally, there are no fees associated with completing or submitting the DD 2870 form itself. However, some healthcare facilities may charge for copying or mailing medical records. It is advisable to inquire about any potential costs when requesting records.
Can I get help with filling out the DD 2870 form?
Yes, assistance is often available for individuals who need help completing the DD 2870 form. Many military healthcare facilities have staff who can provide guidance. Additionally, service members can seek help from their unit’s administrative office or legal assistance office if needed.
Key takeaways
The DD 2870 form is a crucial document used primarily by service members and their dependents to authorize the release of medical information. Understanding how to properly fill out and utilize this form can facilitate better communication and care within the military healthcare system.
- The DD 2870 form is officially titled "Authorization for Disclosure of Medical or Dental Information."
- It is essential for service members to complete this form accurately to ensure their medical records can be shared with authorized personnel.
- One must provide clear identification information, including name, Social Security number, and date of birth.
- The form requires a detailed description of the information that is to be disclosed, ensuring specificity in what is being authorized.
- Signatures are necessary from both the individual authorizing the release and, if applicable, the legal guardian or representative.
- The completed form must be submitted to the appropriate medical facility or organization that holds the records.
- It is advisable to keep a copy of the completed DD 2870 for personal records.
- Service members should be aware of any expiration dates associated with the authorization, as these can limit the duration of the consent.
- In cases of revocation, a new form must be submitted to formally withdraw consent.
- Using the DD 2870 can help ensure that medical providers have access to necessary health information, which is vital for effective treatment.
By adhering to these guidelines, individuals can navigate the process of medical information disclosure with confidence and clarity.
Form Attributes
| Fact Name | Details |
|---|---|
| Purpose | The DD Form 2870 is used to authorize the release of medical records and information. |
| Who Uses It | This form is primarily used by military personnel and their dependents. |
| Governing Law | The release of information is governed by the Health Insurance Portability and Accountability Act (HIPAA). |
| Required Information | Individuals must provide personal details, including name, Social Security number, and contact information. |
| Signature Requirement | A signature is required from the individual authorizing the release of their medical records. |
| Submission Process | The completed form should be submitted to the appropriate medical facility or records office. |
| Validity Period | The authorization remains valid until revoked or until a specified expiration date is reached. |
| Privacy Considerations | All information released is subject to privacy protections under federal law. |
Other PDF Forms
Da 31 Fillable - Requestors should keep a copy of submitted forms for their records.
If you are involved in a boat transaction, it's important to have the necessary documentation to protect your investment. Consider using a reliable resource for your transactions, such as the professional Boat Bill of Sale template, which ensures all details of the sale are properly recorded.
Collision Repair Auto Body Repair Estimate Template - Access a detailed breakdown of repair costs for your vehicle.
Who Can Write Esa Letters - The letter serves to inform housing providers of the necessity of an emotional support animal for the individual’s emotional stability.
Dos and Don'ts
When filling out the DD 2870 form, it is important to follow specific guidelines to ensure accuracy and compliance. Here are some key points to consider:
- Do: Read the instructions carefully before starting the form.
- Do: Provide accurate and complete information in all required fields.
- Do: Use black or blue ink for legibility.
- Do: Double-check your entries for any errors or omissions.
- Don't: Leave any required fields blank.
- Don't: Use abbreviations unless specified in the instructions.
- Don't: Submit the form without reviewing it thoroughly.
- Don't: Forget to sign and date the form before submission.